 Clinical Studies on Tinnitus Pen
Clinical Studies on Tinnitus Pen
Odiomed has been offering Tinnitus Pen to its tinnitus patients since the beginning of 2008 and 2009. We received significant results from our Tinnitus Pen users. 2540 people with chronic tinnitus for over 6 months at a level of effecting their casual life, got Tinnitus Pen from us. Results are as below;
Our patient group consists of 2540 people, 1575 males(%68), 965 females(%32). Age is ranging between 20 to 72 years. Here are the results provided.
| Result |
Patients |
Percentage |
| No more tinnitus |
1168 |
%46 |
| More than %50 relief |
356 |
%14 |
| Less than %50 relief |
229 |
%9 |
| No effect |
787 |
%31 |
| Total |
2540 |
%100 |
1168 users (%46) declared that they do not suffer from tinnitus anymore
356 users (%14) declared that their tinnitus decreased to a level that can easily be ignored
229 users (%9) declared that their tinnitus decreased to a level that enables them to socialize but still have problems in silent environments
787 users (%31) declared that there has been no change with their tinnitus problem.

 Clinical Studies on Tinnitus Treatment System
Clinical Studies on Tinnitus Treatment System
| Alternative Solution In Tinnitus Treatment |
1 |
| Study 1: The Role of LLLT in Treatment of Tinnitus |
1.1 |
| Abstract |
1.1.1 |
| Introduction |
1.1.2 |
| Materials and Methods |
1.1.3 |
| Evaluation |
1.1.4 |
| Discussion |
1.1.5 |
| Conclusion |
1.1.6 |
| Study 2: Comprehensive therapy of patients suffering from tinnitus |
1.2 |
| Study 3: Comprehensive Laser Rehabilitation Therapy of Tinnitus |
1.3 |
| Abstract |
1.3.1 |
| Introduction |
1.3.2 |
| Materials and Methods |
1.3.3 |
| Therapy: LLLT - Physiotherapy aimed at the initial organ of hearing |
1.3.4 |
| Plasebo LLLT |
1.3.5 |
Study 4: Tinnitus and vertigo |
1.4 |
| Study 5: Transmeatal cochlear laser (TCL) treatment of cochlear dysfunction: a feasibility study for chronic tinnitus |
1.5 |
| Study 6: Low-energy laser radiation in the combined treatment of sensorineural hearing loss and Meniere's disease |
1.6 |
| Study 7: Light dosimetry and preliminary clinical results for low level laser therapy in cochlear dysfunction |
1.7 |
| Study 8: Infrared laser applied into the meatus acousticus |
1.8 |
| Study 9: Ex-vivo laser penetration study |
1.9 |
| Study 10: Average duration of tinnitus of 10 years |
1.10 |
| Treatment Protocol |
2 |
| Pre-Examination Evaluation |
2.1 |
| Literature |
3 |
1: Alternative Solution In Tinnitus Treatment Back to top
1.1: Study 1: The Role of LLLT in Treatment of Tinnitus Back to top
Laser Partner, 26.02.2002, Miroslav Prochazka, M.D., Head doctor of the Jarov Rehab Clinic, Prague
1.1.1: Abstract Back to top
Comprehensive laser rehabilitation therapy of tinnitus has proven successful and beneficial for treatment of this widespread civilization disease. Its long-term results are convincing, bringing significant relief to 36 per cent of patients and even leaving remarkable 26 per cent of patients without any symptoms (see Miroslav Prochazka, Ales Hahn: Comprehensive Laser Rehabilitation Therapy of Tinnitus: Long-Term Double Blind Study on a Group of 200 Patients in 3 Years, Laser Partner No. 51/2002). With the results mentioned above we can really speak about a breakthrough. This study brings an additional overview of the role of LLLT (Low Level Laser Therapy) in the treatment. Our results enable us to pinpoint laser as the leading element in the overall therapy of tinnitus.
1.1.2: Introduction Back to top
Tinnitus is an auditory perception appearing without an objective sonic source from the outer environment. Tinnitus can be subjective (heard only by the patient) and objective (sound can be even heard also by others). Our study, however, deals with patients suffering from subjective tinnitus only. According to literature, fifteen per cent of entire population have experienced at least a tinnitus episode some time, its incidence and severity rising with age up to approx. eighty-five per cent of population older than 60. Our clinic has been treating tinnitus for more than 5 years. We have published three studies on this particular issue, and we are of the opinion that our results are being followed in several countries (Brazil, Cyprus, Sweden, Switzerland, Slovakia, Turkey, Japan, Germany etc.) and implemented in numerous clinics with significant results. Studies published by these clinics show results which are almost identical with our experience. Our last study on a group of 200 patients in the course of three years was finalized in February 2002 and published in June 2002. Since there have always been efforts to evaluate an exact role of LLLT in treatment of tinnitus, apart from medication and physiotherapeutic manipulation of neck vertebra as an integral part of the comprehensive therapy, we have decided to create a separate group of patients to be treated only with laser. This was only possible thanks to our vast experience and long involvement in tinnitus treatments.
1.1.3: Materials and Methods Back to top
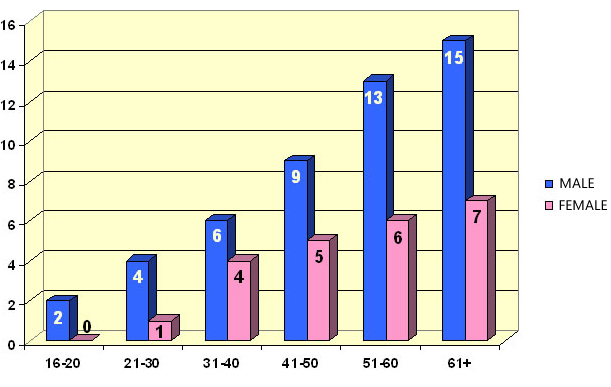
Our group consisted of 72 patients, 49 males, 23 females, age ranging between 16 to 92 years. The age and sex is given in Table 1.
Table 1: Age and Sex Distribution:
| Sex / Age |
16-20 |
21-30 |
31-40 |
41-50 |
51-60 |
61+ |
| Male |
2 |
4 |
6 |
9 |
13 |
15 |
| Female |
0 |
1 |
4 |
4 |
6 |
7 |
| Total |
2 |
5 |
10 |
14 |
19 |
22 |
Graph 1: Age and Sex Distribution:
Prior to the application of LLLT, all the patients underwent the following pre-therapy examination:
1. Anamnesis (aimed especially at the fact whether tinnitus was caused by an acoustic trauma, as well as at genetic predisposition)
2. Subjective evaluation of suffering
3. Clinical examination (otoneurology, axial skeleton, nystagm, blood pressure)
4. Technical examination (audiogram, x-ray of neck vertebra, ENG, tinnitometry)
5. Laboratory testing Audiograms were taken in all the patients prior to the therapy.
After the therapy audiograms were taken in 62.5 per cent, i. e. 45 patients, showing a slight improvement.
Audiogram provides only for numeric range of perception of frequency of sounds, however it does not give us an objective evaluation of quality of hearing. Furthermore, the patients do not see the main improvement in a wider range of frequency of sounds, this remains usually on a similar level, but the main benefit is the absence of the additional burdening sound caused by tinnitus. Therefore the patients can better analyze sounds in general, their hearing is “refreshed” as they usually describe the result of the therapy. Typical audiograms of patients with tinnitus before and after therapy.
Laser device with an infrared laser probe (830 nm) and power output 300 mW was used for the study. The following application dosages and frequency modulations were applied on the following points:
1. meatus acusticus externus - in the direction of the axis of the auditory duct - continuous beam 50 J/cm? followed by 25 J/cm?, frequency modulation of 5 Hz,
2. processus mastoideus - directed on the center, the vector of the beam in the direction of counter lateral orbit, continuous beam 90 J/cm? , followed by 45 J/cm? with 5 Hz pulse frequency.
We strictly appeal to maintain the direction of the vector of aiming the beam - in fact the target structure of the helix is a shape of several square millimetres.
At the beginning, attendance was scheduled to 10 procedures in total, twice a week. Having completed the first series, patients returned after 2 - 3 months for another two series, each consisting of 5 - 6 therapies, once a week.
1.1.4: Evaluation Back to top
Level of subjective complaints was evaluated according to three scales:
Percentage scale - complaints evaluated 100 per cent at the beginning of therapy (Blue), according to the level of relief decreased (Green) to 80, 70 etc. per cent, possible acceleration of problems (Red) goes up to 110, 120 etc. per cent, no tinnitus equals 0 per cent.
Five-grade scale - Five-grade scale - analogous to pain scales;
Reaching from Gr. I = No tinnitus to Gr. 5 = tinnitus interfering all activities;
Grade I = No tinnitus
Grade II = No interfering sound perceived during the day, only in evenings, causing no discomfort
Grade III = Interfering sound perceived during the day, interrupting drowse only
Grade IV = Interrupting drowse and sleep, interfering sound causing discomfort during the day
Grade V = Unbearable discomfort, interfering all activities
Graphic scale – Patient marking 0 to 10, accompanied by a simple graphics showing face grimaces according to his/her amount of subjective hardship. In order to simplify the effect of therapy as much as possible the results were divided in four groups:
1. Patients with no effect of comprehensive therapy
2. Less than 50 per cent relief
3. More than 50 per cent relief
4. No more tinnitus, patient free of the disease.
This evaluation is identical with our previous study, and it enabled us to compare easily the results of both studies.
Table 2: The Role of LLLT in Tinnitus Treatment - Result:
| Result |
Patients |
Percent |
| No effect |
15 people |
%20,8 |
| Less than 50 % relief |
19 people |
%26,4 |
| More than 50 % relief |
22 people |
%30,6 |
| No more tinnitus |
16 people |
%22,2 |
| Total |
72 people |
%100 |
Diagram 2: The Role of LLLT in Tinnitus Treatment - Result:

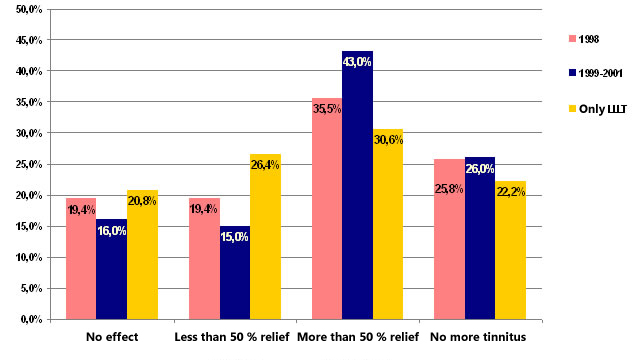
It was interesting to compare our latest results (LLLT only) with those of our previous studies, i. e. our study made in 1998, long-term study between 1999 - 2001, and the initial study aimed at LLLT only.
Table 3: Comparative Results:
| Result |
1998 |
1999-2001 |
only LLLT |
| No effect |
%19,4 |
%16,0 |
%20,8 |
| Less than 50 % relief |
%19,4 |
%15,0 |
%26,4 |
| More than 50 % relief |
%35,5 |
%43,0 |
%30,6 |
| No more tinnitus |
%25,8 |
%26,0 |
%22,2 |
Diagram 3: Comparative Results:
1.1.5: Discussion Back to top
Hippocratic Oath orders us to treat patients to the best of our knowledge and ability. Since our longterm experience in comprehensive treatment of tinnitus has been based on the triad of physiotherapeutic manipulation, medication, and LLLT, we were at a loss whether we would not harm our patients in a way, giving them only a part of the treatment, mere LLLT. We have to declare, that we have selected patients during the introductory examination, sorting out patients whose x-ray indicated a possibility of tinnitus caused by vertebral blockades. On the other hand, this selection led to a more pure evaluation of the role of LLLT in the treatment of tinnitus, leaving out both a possible cause and a corresponding treatment. We have been positively surprised that in general the ratio of individual four groups remained similar. The number of patients with no effect of LLLT slightly increased (by 4.8 per cent when compared to the long-term study, by 1.4 per cent in comparison to the original study of 1998). This is obviously caused by the absence of medication and physiotherapy, showing their supportive effect. In the group evaluating improvement as less than 50 per cent the leading role of LLLT can be evidenced best. More than one-fourth of all patients (26.4) report improvement after therapy performed with LLLT only, which is a result better than those in both previous studies (19.4 and 15.0) . Impressive results have also been obtained in the last two groups , when we imagine more than one half of all patients reporting significant and/or total relief of tinnitus (30.6 + 22.2 = 52.8 per cent).
1.1.6: Conclusion Back to top
22.2 per cent patients suffering from tinnitus never more after treatment with therapeutic laser is a great success of LLLT. It only confirms the leading role of LLLT within comprehensive laser rehabilitation therapy of tinnitus. On the other hand we must stress the necessity to apply the two remaining parts of our therapeutic triad as well, since medication and physiotherapeutic manipulation are integral parts of the general care of our patients, and we should not deprive the suffering of the means and methods capable of bringing them more relief, which we are aware of.
1.2: Study 2: Comprehensive therapy of patients suffering from tinnitus Back to top
Prochazka M, Tejnska R.
37 patients suffering from tinnitus (age 18-86 years) were treated in three ways:
1. Rehabilitation: mobilisation, physical training, physiotherapy.
2. Same as 1 but with placebo laser added.
3. Same as 1 but with functional laser added.
Laser used was 830 nm 300 mW. 2-3 treatments per week were given, total 10 treatments.
Treatment protocol:
- 90 J/cm? CW on mastoideus, 45 J/cm? 5 Hz on mastoideus,
- 50 J/cm? CW on acoustic duct, 25 J/cm? 5 Hz on acoustic duct,
- Tebokan Egb 761 ginko medication was added to treatment.
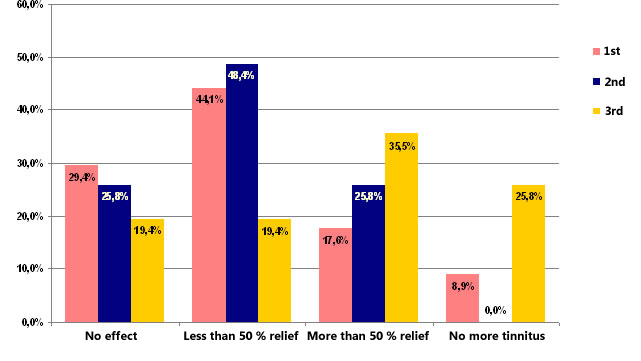
Results were classified as no effect/less than 50% relief/more than 50% relief/no more tinnitus.
Table 4: The percent wise outcome for the three groups:
| Result |
Group 1 |
Group 2 |
Group 3 |
| No effect |
%29,4 |
%25,8 |
%19,4 |
| Less than 50 % relief |
%44,1 |
%48,4 |
%19,4 |
| More than 50 % relief |
%17,6 |
%25,8 |
%35,5 |
| No more tinnitus |
%8,9 |
%0,0 |
%25,8 |
Diagram 4: The percent wise outcome for the three groups:
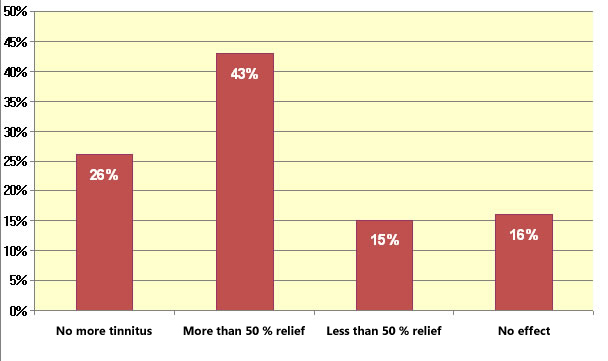
In an extended study over 3 years Prochazka [1263] evaluated the effect of laser in a group of 200 patients. These patients were taking gingko biloba preparations (73%) or Betahistadine (39%) and also had physical therapy, mainly directed at the neck vertebrae. Laser therapy was performed with a 300 mW GaAlAs laser, 75 J/cm? into the ear and 135 J/cm? behind the ear. The outcome can be examined from Table 5.
Table 5: Results of Extended Study:
| Result |
Percent |
| No more tinnitus |
%26 |
| More than 50 % relief |
%43 |
| Less than 50 % relief |
%15 |
| No effect |
%16 |
Diagram 5: Results of Extended Study:
In addition a group of 31 patients were selected for a double blind study where the same therapy as above was performed, but one group received placebo laser. At 6 months the outcome was as follows;
Table 6: Results of the Double-Blind Study:
| Result |
With Laser |
No Laser |
| No more tinnitus |
%25,8 |
%0,0 |
| More than 50 % relief |
%35,5 |
%25,8 |
| Less than 50 % relief |
%19,4 |
%48,4 |
| No effect |
%19,4 |
%25,8 |
Diagram 6: Results of the Double-Blind Study:

1.3: Study 3: Comprehensive Laser Rehabilitation Therapy of Tinnitus Back to top
Edited under official scientific support of EMLA (European Medical Laser Association)
Comprehensive Laser Rehabilitation Therapy of Tinnitus:
Long-Term Double Blind Study in a Group of 200 Patients in 3 Years
M. Prochazka, M.D., Rehab Clinic "Jarov", Prague, CZ
Ass. prof. A. Hahn, ENT Clinic, FNKV Faculty Hospital, Prague, CZ
1.3.1: Abstract Back to top
Definition of tinnitus records that it is an auditory perception for which there is no objective sonic source from the outer environment. Our original study, published in Laser Partner Clinixperience No. 4/2000, has been regarded as a classical tinnitus work. It unambiguously confirmed clinical experience of our predecessors, presented with a high amount of personal enthusiasm (Shiomi, Wilden) but, unfortunately, not much based on statistics. However, recently our study has gained corroboration by originally slightly sceptical medical authorities obtaining statistically almost identical results. Our study has been published more than two years ago. With the time passing by we have been under the impression that the results might be even better than those obtained during several-months therapy in the original cohort of patients. This impression led to a decission that a new comparison with a larger group of patients, than the original forty in our basic study, and followed in a longer time horizon, might be of a certain interest. We were wondering whether our clinical observations, confirmed by personal experience of other clinics, would also find an adequate correlate in statistical expression. A model protocol as well as instruction photographs are attached to the paper.
1.3.2: Introduction Back to top
For our New Study the patients registered in our clinic due to tinnitus for more than three years were chosen. With regard to maximum objectiveness, the patients who had finished attendance due to unknown reasons were included in the "no-effect" group, although we are well aware that a part of them finished the treatment because of various other reasons (such as time cunsuming engagements, problematic transport, family reasons). In a small group of 5 patients we tried to check the objective reasons by a phone query, and indeed, 2 patients gave other reasons whilst 3 patients had finished attendance due to unsatisfactory or no result of procedures. Even though it is interesting for us to have another little group of 6 patients visiting our clinic for check ups and for a series of therapies despite (after a year and more) zero effect of procedures. In a part of this group (in 3 patients) a certain subjective improvement (up to less than 50 per cent relief) can be noticed after a long attendance (2 - 3 years). There is certainly a point at issue, to what an extent this subjective improvement can be regarded as an objective one, whether these patients have not settled down to their complaint... It is a problem of little numbers, definitely not having any influence over the total figure, however, from a clinical point of view we consider this observation interesting... It should be also mentioned that, in general, compliance of patients suffering from tinnitus is excellent, which may be caused by the level of their subjective tribulations leading to a craving to get rid of it.
1.3.3: Materials and Methods Back to top
We have evaluated in total 200 patients visiting our clinic since 1997 till now for tinnitus, followed till 2001, i.e. at least for 3 years. With our approval 8 patients, who were totally free of tinnitus after a short period of treatment, were crossed off and finished attendance earlier. In this respect we have an odd case history of a female patient, who was relieved of her several years lasting lateralized tinnitus after a single mobilization of distal C vertebra (note that entire 8.8 per cent of patients in our original study were relieved of tinnitus only by mere physiotherapy procedures aimed at axial skeleton - there really exists an often disputed diagnosis of vertebrally conditioned tinnitus). As it can be seen above, patients, who finished the therapy due to reasons unknown, have been incorporated in the group "therapy with no effect".
Table 7: Distribution of Sex and Age among the Patients:
| Age |
0-15 |
15-25 |
25-35 |
35-45 |
45-55 |
55-65 |
65-75 |
75+ |
Total |
| Male |
2 |
3 |
9 |
11 |
23 |
28 |
32 |
4 |
112 |
| Female |
0 |
4 |
7 |
16 |
19 |
25 |
16 |
1 |
88 |
| Total |
2 |
7 |
16 |
27 |
42 |
53 |
48 |
5 |
200 |
Diagram 7: Distribution of Sex and Age among the Patients:
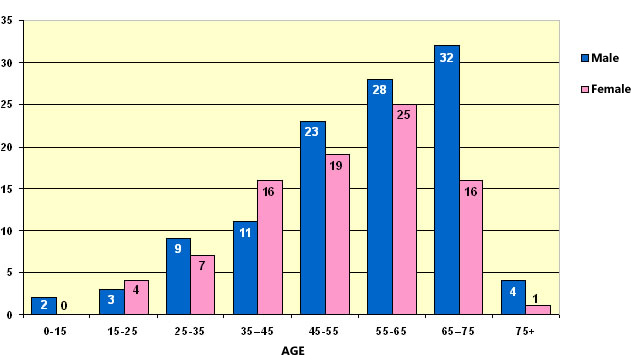
Our group (New Group) of patients consisted of 112 males and 88 females (in comparison with our previous study there was an interesting shift towards higher share of males, according to our opinion this more corresponds with the level of distribution of tinnitus within population in relation to work anamnesis and hobbies). Average age was 64 years, ranging within the limits of 15 and 98 years. This meant a shift towards higer categories of age, probably corresponding with the incidence of tinnitus within the population, and maybe also due to the fact that our activities have been covered by media, mainly by those focussed on seniors, and thus new patients could have appeared on the basis of media influence.
Level of subjective complaints was evaluated according to, nowadays almost classical, three scales:
1. Percentage Scale (complaints evaluated 100 per cent at the beginning of therapy, according to the level of relief decreased to 80, 70 per cen, possible acceleration of problems goes up to 110, 120 per cent, no tinnitus equals 0 per cent),
2. Five-grade scale - nalogous to pain scales (I = no tinnitus, V = tinnitus limiting all activities, II, III and IV = clearly defined complaints)
Grade I = No tinnitus
Grade II = No interfering sound perceived during the day, only in evenings, causing no discomfort
Grade III = Interfering sound perceived during the day, interrupting drowse only
Grade IV = Interrupting drowse and sleep, interfering sound causing discomfort during the day
Grade V = Unbearable discomfort, interfering all activities
3. Graphic scale – patient marking 0 to 10, accompanied by a simple graphics showing face grimaces according to his/her amount of subjective hardship
This combination has proven more than suitable for evaluating such a subjective suffering as tinnitus. Particularly nowadays, when most clinical studies are aimed at evaluation of "quality of life" of individual patients, this combination appears a good criterion to measure such a most valuable state. Above mentioned combination can also make a serious processing possible, with regard to different social, economic, expressive, cultural and intelectual qualities of individual patients.
In order to simplify the effect of therapy as much as possible the results were divided in four groups:
1- Patients with no effect of comprehensive therapy (or even with aggravated condition, however we can say that no patient has reported a setback of tinnitus after the therapy)
2- Less than 50 per cent relief as far as subjective evaluation of the patient is concerned
3- More than 50 per cent relief as far as subjective evaluation of the patient is concerned
4- No more tinnitus, patient free of the disease.
This evaluation is identical with our previous study, and it enabled us to compare easily the results of both studies.
1.3.4: Therapy: LLLT - Physiotherapy aimed at the initial organ of hearing Back to top
LLLT - Physiotherapy aimed at the initial organ of hearing
There is no need to discuss necessary parameters of laser probes used. We need an infrared laser beam with a sufficient power output (we have been using an IR 300 mW laser probe, we also tried using a 450 mW probe but a part of our patients reported a subjectively unpleasant thermic effect in the area of application). On the other hand, we pay maximum attention to irradiation of a sufficient dosage of energy.
In our clinic we use the following techniques of LLLT application:
1. application on meatus acusticus externus - in the direction of the axis of the auditory duct - continuous beam 50 J/cm? followed by 25 J/cm?, frequency modulation of 5 Hz,
2. irradiation of processus mastoideus - directed on the center, the vector of the beam in the direction of counterlateral orbit, continuous beam 90 J/cm? , followed by 45 J/cm? with 5 Hz pulse frequency.
Modulation of 5 Hz we use due to assumed potenciation of stimulative effect of non-invasive laser.
We strictly appeal to maintain the direction of the vector of aiming the beam - in fact the target structure of the helix is a shape of several square milimeters. It might be the reason why, when compared with other laser devices with the same output parameters, therapy with CCM probes has proved rather successful due to their characteristic diffusion of the emitted beam, increasing probability of hitting desired target structures (difference of prognostic level of success between hitting the target with a shotgun or with a rifle - thanks to ass. prof. Horak for his witty comparison). LLLT has been applied on 100 per cent of our patients.
Attendance was scheduled so that the first series of 8 - 10 procedures in total, twice a week, be a complex consisting of medication, rehabilitation therapy of axial skeleton, and LLLT. In the interval of 2 - 3 months further courses of therapy follow, usually consisting of 5 - 6 therapies, once a week, always as a series of LLLT procedures. Therapy of axial skeleton is added when necessary (often not necessary in case of regularly exercising patients, instructed properly in the course of the first series). Medication with Egb 761 continuing in the long term, most of the patients after several months of therapy with a reduced dosage 1 - 0 - 1 tablets, in the order of at least several more months. A part of the patients in the cycle between procedures has noticed a possibility to titrate medication according to immediate subjective complaints - it means they keep to regular dosage 1 - 0 - 0, when tinnitus accelerates switching to 1 - 1 - 0, or even to 1 - 1 - 1 tablets. Possible episodes of accelerated tinnitus usually abate quickly then. In case of long term stabilized patients we plan clinical check ups at least twice a year, always connected with mobilisation of acute blockades of distal C vertebra. Inviting patients for these check ups always in the spring and fall has proved successful.
We have noticed one rather substantial phenomenon of LLLT: so far no side effect has been reported. On the other hand, there is an interesting clinical finding in a certain group of patients (6 patients = 3 per cent), an acceleration of tinnitus after the first few LLLT procedures. Positive aspect of this phenomenon is that these patients have always belonged in the group with a massive effect of the therapy (more than 50 per cent relief, or even free of tinnitus at all). This clinical observation has been personally confirmed by other authors working at tinnitus treatment with the use of LLLT (Wilden).
1.3.5: Plasebo LLLT Back to top
Due to persistently appearing theories on the effect of LLLT of tinnitus being a mere placebo we have created a minor group of 31 patients in order to confirm or exclude this hypothesis. In the course of three months attendance these patients underwent medication therapy as well as physiotherapy of axial skeleton with classical rehabilitation techniques in the same extent as all the other patients did. Instead of a functional laser source these patients were treated with a probe not emitting laser beam, although there was acoustic as well as visual signalization of operation. Among all other physiotherapeutic devices a non-invasive laser is extremely suitable to perform a placebo test, since its application on a patient is not connected with any subjective feelings nor phenomenons (in contradiction to electrotherapy, for instance). As we work with an IR wavelength, it was possible to arrange a double blind study, for the fact whether the therapist works with a device emitting laser beam or with a placebo unit was not even known to the therapeutic personnel.
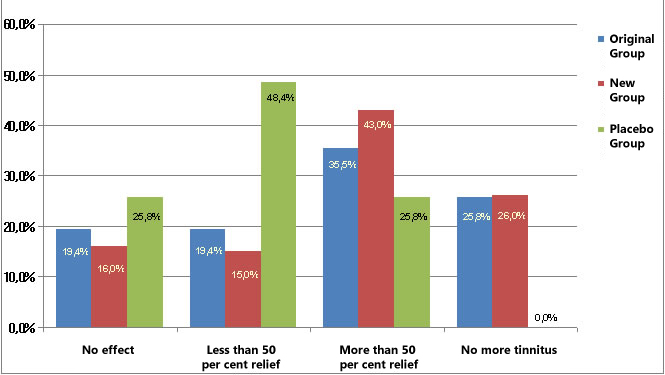
The results -unambiguously confirming that there is no placebo involved in LLLT- are summarized in Table 8. The outcome is undoubtedly statistically significant.
Table 8: Results of Placebo Test:
|
Effect of Therapy |
Original Group
(31 patients-6 months) |
New Group
(200 patients-3 years) |
Placebo Group
(31 patients-3 months) |
|
No effect |
19.4 % |
16.0 % |
25.8 % |
|
Less than 50 per cent relief |
19.4 % |
15.0 % |
48.4 % |
|
More than 50 per cent relief |
35.5 % |
43.0 % |
25.8 % |
|
No more tinnitus |
25.8 % |
26.0 % |
0.0 % |
Diagram 8: Results of Placebo Test:
1.4: Study 4: Tinnitus and vertigo Back to top
Jan Tunér, DDS Laser-Medical Society Grängesberg, Sweden
A new and promising indication for laser therapy is tinnitus.
This inner ear disease is a growing problem in noisy modern society and the number of persons suffering from tinnitus is increasing. Traditional treatment for tinnitus is psychological support or various masking procedures. Acupuncture and ginko extracts have been tried with limited success. Laser therapy alone offers a new and promising treatment modality. The correlation between tinnitus/vertigo and cranomandibular disorders (CMD) has been known for quite some time, yet few dentists seem to be aware of this. It is not natural for the dentist to ask, nor for the patient to inform the dentist about such a situation since it does not appear to be a dental indication. However, quite a number of tinnitus/vertigo patients will be relieved of their symptoms if a proper CMD treatment is performed. Low level lasers have been used to treat tinnitus patients with reasonable success, if sufficient energy and suitable treatment technique is used. These lasers have also proved themselves successful in the treatment of CMD. It is obvious, therefore, that low level laser therapy is an appropriate treatment modality for the yet undefined subgroup of tinnitus/vertigo patients with a CMD background. Laser therapy will reduce pain levels, ease muscular spasms and revert the vicious circle.
1.5: Study 5: Transmeatal cochlear laser (TCL) treatment of cochlear dysfunction: a feasibility study for chronic tinnitus Back to top
Tauber S, Schorn K, Beyer W, Baumgartner R., Department of Otolaryngology, Ludwig-Maximilians- University of Munich
Low-level-laser-therapy (LLLT) targeting the inner ear has been discussed as a therapeutic procedure for cochlear dysfunction such as chronic cochlear tinnitus or sensorineural hearing loss.
Former studies demonstrate dose-dependent biological and physiological effects of LLLT such as enhanced recovery of peripheral nerve injuries, which could be of therapeutic interest in cochlear dysfunction. To date, in patients with chronic tinnitus mastoidal and transmeatal irradiation has been performed without systematic dosimetric assessment. However, light-dosimetric studies on human temporal bones demonstrated that controlled application of laser light to the human cochlea depends on defined radiator position within the external auditory meatus. This feasibility study first presents a laser application system enabling dose-controlled transmeatal cochlear laser-irradiation (TCL), as well as preliminary clinical results in patients with chronic cochlear tinnitus.
Tauber S, Schorn K, Beyer W, Baumgartner R., Department of Otolaryngology, Ludwig-Maximilians- University of Munich
The novel laser TCL-system, consisting of four diode lasers (lambda=635 nm-830 nm) and a new specific head-set applicator, was developed on the basis of dosimetric data from a former light-dosimetric study. In a preliminary clinical study, the TCL-system was applied to 35 patients with chronic tinnitus and sensorineural hearing loss. The chronic symptoms persisted after standard therapeutic procedures for at least six months, while retrocochlear or middleear pathologies have been ruled out. The patients were randomised and received five single diode laser treatments (lambda=635 nm, 7.8 mW cw, n=17 and lambda=830 nm, 20 mW cw, n=18) with a space irradiation of 4 J/cm? site of maximal cochlear injury. For evaluation of laser-induced effects complete otolaryngologic examinations with audiometry, tinnitus masking and matching, and a tinnitus- self-assessment were performed before, during and after the laser-irradiation. The first clinical use of the TCL-system has been well tolerated without side-effects and produced no observable damage to the external, middle or inner ear. Changes of tinnitus loudness and tinnitus matching have been described. After a follow-up period of six months tinnitus loudness was attenuated in 13 of 35 irradiated patients, while two of 35 patients reported their tinnitus as totally absent. Hearing threshold levels and middle ear function remained unchanged. Further investigations by large double-blind placebo controlled studies are mandatory for clinical evaluation of the presented TCL-system and its therapeutic effectiveness in acute and chronic cochlear dysfunction.
1.6: Study 6: Low-energy laser radiation in the combined treatment of sensorineural hearing loss and Meniere's disease Back to top
Low-energy laser radiation in the combined treatment of sensorineural hearing loss and Meniere's disease;
Pal'chun VT, Lapchenko AS, Kadymova MI, Kucherov AG.
59 patients with neurosensory hypoacusis and 45 with Meniere's disease underwent helium-neon laser intra- or supravascular radiation of blood. The treatment proved effective in acute neurosensory hypoacusis and Meniere's disease. Light dosimetry and preliminary clinical results for low level laser therapy in cochlear dysfunction
1.7: Study 7: Light dosimetry and preliminary clinical results for low level laser therapy in cochlear dysfunction Back to top
Light dosimetry and preliminary clinical results for low level laser therapy in cochlear dysfunction
Beyer W et al.
The light distribution inside the cochlear windings produced by irradiation of the tympanic membrane was quantitatively measured ex vivo for wavelengths of 593, 612, 635, 690, 780 and 805 nm by means of video dosimetry. The transmission of light across the tympanic cavity and the promontory depends strongly on the wavelength. Spatial intensity variations of a factor of 10 and more inside the cochlear windings have been measured. The clinical study was performed with 30 patients suffering from chronic permanent tinnitus. 5 irradiations within 2 weeks each with a space irradiation of 4J/cm? were applied at the cochlear position to be treated. Diode lasers of 635 or 830 nm, 15 patients each, were used. During and after irradiation there was no significant change of hearing. However, 40% of the patients reported a slight to significant attenuation of the tinnitus loudness of the treated ear. There was no difference between the two wavelength groups.
1.8: Study 8: Infrared laser applied into the meatus acousticus Back to top
Dr. Shiomi [686] has investigated the effect of infrared laser applied directly into the meatus acousticus, 21 J, once a week for 10 weeks.
The result of this non-controlled study is as follows: 26% of the patients reported improved duration, 58% reduced loudness and 55% reported a general reduction in annoyance. The same author [687] has also examined the effect of light on the cochlea using guinea pigs. Direct laser irradiation was administered to the cochlea through the round window. The amplitude of CAP was reduced to 53-83% immediately after the onset of irradiation. The amplitude then returned to the original level. The results of this investigation suggest that laser therapy might lessen tinnitus by suppressing the abnormal excitation of the eighth nerve of the organ of Corti.
1.9: Study 9: Ex-vivo laser penetration study Back to top
Dr. Tauber [1091] has performed an ex-vivo laser penetration study. Based on these findings it was possible to calculate the energy needed to obtain a dose of 4 J/cm? in the cochlea itself.
Irradiation via the mastoid showed values 103 to 105 times smaller (depending on wavelength) than irradiation through the tympanic membrane. 30 patients were treated five times within 2 weeks. One group was irradiated with 635 nm diode laser, the other with 830 nm diode laser. By self-assessment around 40% of the patients reported a slight to significant attenuation of the tinnitus loudness of the irradiated ear.
1.10: Study 10: Average duration of tinnitus of 10 years Back to top
Dr. Hahn [1310] examined 120 patients with an average duration of tinnitus of 10 years. The patients underwent puretone audiometry, speech audiometry and objective audiometry tests. The intensity and frequency of tinnitus was also determined. EGb 761 was administered 3 weeks before the start of laser therapy. The patients underwent 10 sessions of laser therapy, each lasting 10 minutes. An improvement in tinnitus was audiometrically confirmed in 50.8% of the patients; 10 dB in 18, 20 dB in 22, 30 dB in 10, 40 dB in 6 and 50 dB in 5 patients.
|
Decrease in Tinnitus |
10 dB |
20 dB |
30 dB |
40 dB |
50 dB |
|
Patients |
18 |
22 |
10 |
6 |
5 |
2.1: Pre-Examination Evaluation Back to top
|
Co-operation between specialists
|
-neurology
-ear-nose-throat
-rehabilitation (or physiotherapy) |
|
Gathering anamnesic data |
Acoustic trauma in the anamnesis (regardless to one-time episode or a chronic burden) |
|
Abuse of potentially ototoxic medicaments (especially antibiotics, total anesthesia) |
|
Ocurrence of tinnitus in family anamnesis |
|
Clinical examination |
Thorough otoneurological examination |
|
Thorough examination of axial skeleton |
|
Nystagmus |
|
Blood pressure |
|
Technical means of examination |
Audiogram + masking of tinnitus |
|
CT/NMR |
|
X-ray of C vertebra |
|
ENG |
|
Tinnitogram |
|
Lab tests |
Especially detection of diabetes mellitus |
|
Lipid metabolism disorders |
|
Functional pathology of axial skeleton |
Patients should always be examined by a specialist on myoskeletal medicine |
3: Literature Back to top
|
Indication
|
Author |
Name of Publication |
Date |
Title |
|
Innenohrstörungen |
U. Witt
C. Felix |
Selective photo-biochemotherapy in the combination of laser and gingkoplan extracts |
1989 |
Selektive photo-Biochemotherapie in der Kombination Laser und Ginko-Pflanzenektrakt
nach der Methode Witt (unpublished material) |
|
Hearing loss
and tinnitus |
P. Plath
J. Oliver |
Adv. Otorhinolaryngol. 1995;
49:101-4 |
1995 |
Results of combined low-power laser therapy and extracts of Ginko biloba in cases of sensorineural hearing loss and tinnitus |
|
Irradiation on
tinnitus |
Y. Shiomi
H. Takahashi
I. Honjo |
Auris Nasus Larynx 1997;24(1):39-42 |
1997 |
Efficacy of transmeatal low power laser irradiation on tinnitus (a preliminary report) |
|
Irradiation on
inner ear |
Y. Shiomi |
Pract Otol (Kyoto) 1994; 87: 1135-1140 |
1994 |
Effect of low power laser irradiation on inner ear (in Japanese) |
|
Tinnitus
Therapy |
A. Hahn
I. Sejna
k. Stoblova |
Acta Otolaryngol 2001, 545, 92-93 |
2001 |
Combined Laser-Egb 761 Tinnitus Therapy |
|
Tinnitus |
M. Prochazka
R. Tejnska |
Proc. Laser Florence 99 |
1999 |
Comprehensive therapy of patients suffering from Tinnitus |
|
Neurootoligische Erkrankungen |
R. Swoboda
A. Schott |
Treatment of neurotologic diseases with Gingko biloba and low level laser therapy |
1992 |
Behandlung neurootologischer Erkrankungen mit Ginko biloba Hevert, Hyperforat und low-Power-Laser-Therapy (Medizinische Akademie Erfurt) |
|
Chronic tinnitus |
H. Wedel
L. Calero
M. Walger |
Soft-laser/Gingko therapy in chronic Tinnitus. Adv Otorhinolaryngol. 1995;49:105-8 |
1995 |
Soft-laser/Gingko therapy in chronic Tinnitus (a placebo controlled study) |
|
Treatment of
tinnitus |
F. Mirz
R. Zachariae
S. Andersen |
The low-power laser in the treatment of tinnitus. Clin
Otolaryngol 1999; 24: 346-354 |
1999 |
The low-power laser in the treatment of tinnitus |
|
Cochlear
dysfunction |
W. Beyer |
Light dosimetry and preliminary clinical results for low level laser therapy in cochlear disfunction.
Proc. Laser Florence 99 |
1999 |
Light dosimetry and preliminary clinical results for low level laser therapy in cochlear disfunction |
|
Laser
irradiation of
the cochlea |
S. Tauber
R. Baumgartner
K. Schorn |
Experimental study for laser irradiation of the cochlea. Lasers
Surg Med 2001;28:(1):18-26 |
2001 |
Lightdosimetric quantitative analysis of the human petrous bone |
|
Der Körper des
Menschen |
Adolf Faller |
Der Körper des Menschen, Thieme Verlag 1995 |
1995 |
Der Körper des Menschen |
|
Low Level Laser
Application |
H. Walter
A. Walter |
Photobiological Basics of Low Level Laser Application. Dt. Z. für Akupunktur 2/97 |
1997 |
Low Level Laser Application |
|
Low-Power
Laser Therapy |
T. Karu |
Photobiology of Low-Power Laser Therapy, Harwood Academic Publishers, New York 1989 |
1989 |
Photobiology of Low-Power Laser Therapy |
|
Tinnitus |
Olivier J.
Plath P. |
Laser Therapy, 5:137-139, 1993, John Wiley & Sons, Ltd. |
1993 |
Combined low power laser therapy and extracts of Ginkgo |

 English
English
 Türkçe
Türkçe Deutsch
Deutsch العربية
العربية